A patient in a rural county logs into a video call at 8 a.m. and sees a cardiologist by 8:15, no three-hour drive required. A clinic cuts its no-show rate by nearly a third just by moving follow-ups online.
It’s what’s already happening at scale, and it’s why “should we build a telemedicine app” has quietly turned into “how do we build one that actually works”, and how to choose the right telemedicine or healthcare app development company.
The hard part is the build itself: getting the architecture right, staying HIPAA-compliant without slowing engineering to a crawl, choosing a tech stack that won’t need a rebuild in two years, and connecting cleanly to systems like Epic or Cerner.
CMS’s more than 250 codes are now reimbursable, so the reimbursement uncertainty that made health systems hesitate for years is largely gone. What’s left is an execution problem.
This guide walks through exactly about telemedicine app development: the architecture, the real costs, the compliance work, the technology decisions, and what separates a platform that scales from one that quietly stalls after launch.
What Is Telemedicine App Development?
Telemedicine app development is the process of designing and building software that lets patients and licensed providers conduct clinical visits remotely, through video, messaging, or monitoring. It differs from general health app development because it must support licensed care delivery, not just data tracking.
Why it’s a different discipline than consumer app development
A wellness or fitness app collects health-adjacent data casually, with no licensed clinician on the other end and no requirement to hold up in a HIPAA audit. A telemedicine platform sits in a different category entirely. It has to verify identity on both sides of a consultation, protect protected health information (PHI) under active clinical use, support e-prescribing tied to controlled-substance regulations, and produce documentation that becomes part of a patient’s permanent medical record.
Those requirements shape the technical architecture from the first design decision, not as an afterthought before launch.
The Four Systems that Make up a Telemedicine Platform
A production-grade platform is built from four interconnected systems, not a single app:
- Patient application — scheduling, video visits, secure messaging, and payment
- Provider portal — consultation workspace, clinical notes, e-prescribing, and patient history
- Admin dashboard — user management, compliance monitoring, and reporting
- Backend and compliance layer — the APIs and infrastructure connecting scheduling, video, EHR data exchange, and payments, wrapped in encryption and access controls that apply across all three front-end systems
What Features Should a Telemedicine App Include?
A telemedicine app needs four feature categories: MVP essentials for care delivery, advanced features for differentiation, provider-facing clinical tools, and admin infrastructure.
Feature selection should follow the actual clinical workflow of the organization building the app, not a generic industry checklist.
1. MVP essentials
| Feature | Why it exists |
| Secure registration and MFA login | Healthcare platforms are frequent targets for credential-based attacks; multi-factor authentication is the baseline before any PHI is exposed |
| User profiles | Scheduling, billing, and prescribing all depend on accurate demographic and insurance data |
| Doctor discovery | Lets patients filter by specialty, language, and insurance network instead of browsing an undifferentiated directory |
| Appointment scheduling | Reconciles provider calendars in real time to prevent double-booking across time zones and recurring availability blocks |
| Secure video consultations | The clinical core of the platform; requires encrypted transport and adaptive bitrate streaming for unstable connections |
| Secure messaging | Supports asynchronous follow-up on lab results or medication questions without a full visit |
| E-prescriptions | Routes prescriptions through pharmacy networks using the NCPDP SCRIPT standard, reducing transcription errors common with phoned-in orders |
| EHR read access | Gives providers patient history instead of starting each virtual visit from a blank chart |
| Payment processing | Handles insurance verification, co-pay collection, and HSA/FSA card processing |
| Push notifications | Reduces appointment no-shows through reminders |
Each of these solves a specific operational problem rather than existing for feature-count purposes.
2. Advanced features worth adding once volume justifies them
AI symptom assessment and AI-assisted clinical documentation reduce clinician charting time, a well-documented driver of burnout, but they need enough historical visit data to tune accurately. Deploying either on sparse data tends to create more liability than efficiency.
Remote patient monitoring (RPM) and wearable integrations extend the platform beyond episodic visits into continuous chronic-disease management, such as the area where telemedicine’s cost and outcome advantages are strongest.
RPM requires new backend infrastructure for continuous data ingestion and clinical alerting, which is a materially different engineering problem than scheduled video visits.
Voice assistants, multi-language support, and predictive analytics dashboards extend access to older patients and non-English-speaking populations, and help provider organizations flag at-risk patients before an acute event rather than after one.
3. Provider-facing features
Providers need calendar management with block scheduling, a consultation workspace that surfaces patient history alongside the live video feed, structured clinical note templates, e-prescribing built into the visit flow rather than a separate system, and tools for managing follow-up appointments.
4. Admin features
Administrators need user and role management, a compliance monitoring dashboard that flags access anomalies in real time, revenue and utilization reporting, a lightweight CMS for provider bios and patient education content, and audit logs that hold up to regulatory review.
| Feature | Purpose | Business Value | Patient Benefit |
| Secure video consultations | Deliver real-time clinical care remotely | Reduces facility overhead, widens service radius | Access to care without travel |
| Appointment scheduling | Coordinate provider and patient availability | Reduces administrative staff workload | Predictable, convenient booking |
| E-prescriptions | Route prescriptions electronically to pharmacies | Fewer transcription errors, lower liability | Faster medication access |
| Remote patient monitoring | Continuously track chronic condition indicators | Enables value-based care contracts | Earlier intervention, fewer ER visits |
| AI clinical documentation | Auto-generate visit notes from conversation | Reduces clinician documentation time | More attention during visits |
| Compliance monitoring dashboard | Detect policy violations in real time | Lowers breach and penalty risk | Assurance that data is protected |

How Much Does Telemedicine App Development Cost in 2026?
Telemedicine app development costs range from roughly $40,000 for a narrowly scoped MVP to $500,000 or more for an enterprise platform with EHR integration, AI functionality, and multi-region compliance.
Technical complexity is the primary driver of cost, and the biggest single variable is how much compliance and integration work the platform requires.
What actually drives the price
- Platform choice: Native iOS and Android app development roughly doubles frontend cost compared to a single cross-platform codebase.
- Video infrastructure: Self-hosted WebRTC is cheaper at scale but requires dedicated engineering; managed platforms like Twilio or Agora cut development time but add ongoing per-minute fees.
- Compliance scope: HIPAA-only is a materially smaller project than HIPAA plus GDPR plus state-by-state telehealth licensure requirements.
- EHR integrations: Connecting to Epic or Cerner involves custom FHIR resource mapping, sandbox testing, and the vendor’s own certification process, often adding tens of thousands of dollars per integration before any production traffic flows.
- AI functionality and remote monitoring: Both require additional backend infrastructure for data ingestion and model hosting.
- Security testing: A HIPAA risk assessment and penetration test should be a fixed line item in every project budget, not an optional add-on.
Organizations comparing telemedicine app development solutions should weigh these cost drivers against the platform’s expected lifespan and patient volume, since a system built too leanly for its actual compliance scope tends to require expensive rework within the first year.
| Project Type | Estimated Cost | Typical Timeline | Suitable For |
| Basic MVP | $40,000 – $90,000 | 3–5 months | Solo practices, early-stage validation |
| Mid-sized platform | $90,000 – $250,000 | 5–9 months | Multi-provider clinics, regional networks |
| Enterprise platform | $250,000 – $600,000+ | 9–18 months | Hospital systems, multi-state operators |
These figures cover development only. Hosting, video minute fees, third-party API charges, compliance audits, and maintenance typically add another 15–25% of the initial build cost every year; a number that should be modeled into the business case from the start rather than treated as a rounding error after launch.
How Do You Build a HIPAA-Compliant Telemedicine App?
HIPAA compliance is an architectural approach, not a feature added before launch. It means every component, from database schema to API gateway, is built assuming it will handle protected health information, with encryption, access control, and audit logging designed in from the first line of code.
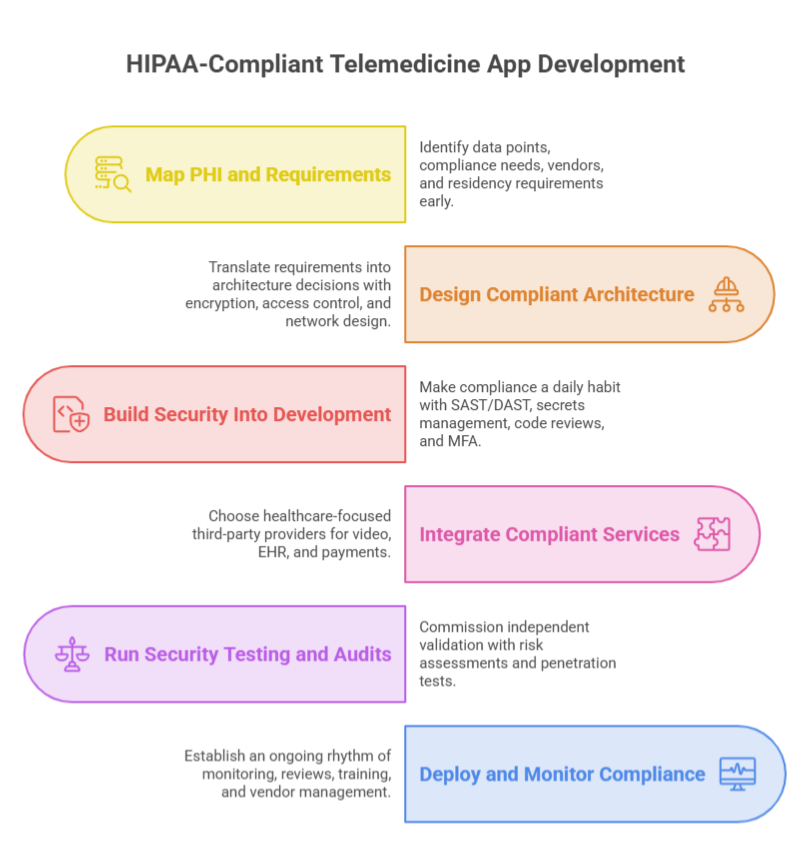
1. Map Your PHI and Compliance Requirements Early
Before any design work starts, list every data point the app will touch, like patient names, diagnoses, insurance IDs, video recordings, chat logs, prescription history, and flag which ones qualify as protected health information (PHI). This shapes everything downstream.
- Identify whether you need HIPAA only, or HIPAA plus GDPR if you’re serving European patients.
- List every third-party vendor that will handle data, including video provider, cloud host, payment processor, SMS service, since each one needs its own Business Associate Agreement (BAA).
- Decide data residency requirements now, not after development starts.
You can also run a lightweight threat-modeling session at this stage, using a framework like STRIDE, to catch design-level risks before they get built into the product.
2. Design a Compliant Architecture
With requirements locked, translate them into concrete architecture decisions before writing any backend code.
- Encryption: AES-256 for data at rest, TLS 1.2 or higher for data in transit.
- Key management: AWS KMS, Azure Key Vault, or Google Cloud KMS.
- Access control: role-based permissions built around HIPAA’s “minimum necessary” standard, mapping each job function to only the data it needs
- Network design: private subnets for any service touching PHI, sitting behind a web application firewall
A signed BAA with AWS, Azure, or Google Cloud only covers the specific services named in it, so confirm exactly which services are covered before you build on top of them.
3. Build Security Into the Development Process
Once development starts, compliance becomes a daily engineering habit, not a milestone.
- Add SAST and DAST scanning (tools like Snyk or Checkmarx) directly into your CI/CD pipeline.
- Store API keys and credentials in a secrets manager like HashiCorp Vault, never in source code.
- Require two reviewer approvals on any pull request touching a PHI-handling module.
- Use synthetic or de-identified data in staging and test environments; never a live PHI copy.
- Enforce MFA on every account type (patient, provider, admin) before login grants access to PHI.
You can also build audit logging in as each feature ships, so every PHI access, who, when, from where, what action, is captured from day one instead of retrofitted later.
4. Integrate Compliant Third-Party Services
Most telemedicine platforms lean on external providers for video, EHR connectivity, and payments. Choose ones built for healthcare from the start.
- Video: Twilio or Zoom SDKs, both offering HIPAA-eligible configurations.
- EHR integration: SMART on FHIR or a connector platform like Redox.
- Payments: Stripe, paired with insurance API integrations for claims.
Test every integration in a sandbox environment first, so you’re never validating a new API connection against live patient data.
Run Security Testing and Compliance Audits
Before go-live, the platform needs independent validation, not a self-assessment.
- Commission a formal HIPAA risk assessment from an assessor outside the build team.
- Run a third-party penetration test simulating real attack scenarios.
- Remediate every finding and re-test to confirm the fix actually worked.
- Confirm every BAA is fully signed before real patient data touches the system.
You can also draft your incident response plan at this stage. HITECH’s breach notification rule requires notifying affected individuals within 60 days of discovering a breach involving unsecured PHI, so the escalation path needs to exist before it’s ever needed.
5. Deploy and Monitor Compliance Post-Launch
Compliance work doesn’t stop at launch. It becomes an ongoing operating rhythm.
- Enable production monitoring and alerting (tools like Datadog or New Relic) to flag unusual access patterns in real time.
- Review access permissions quarterly as staff and roles change.
- Repeat the full risk assessment annually.
- Refresh staff training annually, like human error, not sophisticated hacking, causes most real-world healthcare breaches.
- Add a signed BAA and security review for every new vendor before it touches patient data, not after.
Budget for this ongoing work. Most healthcare platforms allocate 15–20% of the original build cost every year to compliance monitoring, security patches, and audit maintenance.
A Note on GDPR
If the platform serves patients in Europe, GDPR applies alongside or instead of HIPAA. It treats health data as a “special category” requiring explicit consent, grants patients the right to full data erasure, and requires a Data Protection Officer once an organization processes health data at scale. This is a general overview, not legal advice.
Which Technology Stack Is Best for Telemedicine App Development?
The right choice depends on team expertise, expected scale, compliance region, and whether video is core to the product or a secondary feature. Every stack decision is a trade-off between development speed, long-term maintainability, and performance under healthcare-specific constraints.
Frontend
Flutter and React Native allow a single codebase to target iOS and Android, cutting development time roughly in half compared to native builds, at the cost of a small performance gap on camera- and video-intensive screens.
Native development (Swift/Kotlin) removes that gap and gives full access to platform-specific APIs, at the cost of maintaining two separate codebases.
Backend and data
Node.js suits real-time, I/O-heavy workloads like chat and notifications. Java and .NET are common in enterprise healthcare environments already standardized on those ecosystems, with mature tooling but slower iteration speed than a leaner stack.
For data, PostgreSQL is the default for structured clinical and transactional data requiring strong consistency, while MongoDB fits less structured data like activity logs or flexible intake forms.
Video communication
WebRTC is the open standard underlying most solutions, offering full control and no per-minute fees, but requiring in-house signaling and TURN/STUN infrastructure.
Twilio and Agora are managed platforms built on WebRTC that cut time-to-launch and include HIPAA-eligible configurations, in exchange for usage-based costs that scale with visit volume.
Interoperability and identity
HL7, FHIR, and SMART on FHIR are non-negotiable if EHR integration is on the roadmap. These are the protocols Epic, Cerner, and virtually every major EHR vendor build around, typically using FHIR resources like Patient, Appointment, Encounter, and DocumentReference to exchange data.
Authentication should combine OAuth 2.0 for delegated access with mandatory MFA. AI capabilities, such as speech-to-text, clinical documentation assistance, triage support, are increasingly built on third-party medical-grade models rather than trained in-house, given the clinical validation burden of proprietary model development.
| Technology | Primary Use | Advantages | Considerations |
| Flutter / React Native | Cross-platform frontend | Single codebase, faster time-to-market | Slight performance overhead on camera-heavy screens |
| Node.js | Real-time backend services | Strong for concurrent I/O, messaging, notifications | Less suited to CPU-heavy processing |
| PostgreSQL | Structured clinical data | Strong consistency, mature healthcare tooling support | Less flexible for unstructured data |
| WebRTC (self-hosted) | Video infrastructure | No per-minute fees, full control | Requires dedicated infrastructure engineering |
| Twilio / Agora | Managed video infrastructure | Fast to implement, built-in compliance tooling | Ongoing usage-based costs |
| FHIR / SMART on FHIR | EHR interoperability | Industry standard, required for Epic/Cerner integration | Requires certification and mapping effort |
Custom Telemedicine App Development vs. White-Label Solutions
Custom development offers full ownership, flexibility, and long-term scalability at higher upfront cost and longer timelines. White-label solutions offer fast deployment and lower initial cost at the expense of customization and long-term flexibility.
The right choice depends on how differentiated the clinical workflow needs to be and how quickly the organization needs to launch.
| Dimension | Custom Development | White-Label |
| Customization | Fully tailored to workflow | Limited to vendor configuration |
| Ownership | Full code and data ownership | Vendor-controlled architecture |
| Deployment Speed | Slower (months) | Fast (weeks) |
| Scalability | Built for organization-specific scale | Bounded by vendor’s platform limits |
| Compliance Flexibility | Fully controllable | Dependent on vendor’s implementation |
| Long-Term Cost | Higher upfront, lower recurring | Lower upfront, ongoing licensing fees |
| Best Fit | Multi-specialty systems, unique workflows | Single-clinic pilots, rapid market entry |
How Do Telemedicine Apps Integrate with EHR Systems Like Epic and Cerner?
Telemedicine apps integrate with Epic, Cerner, and other EHR systems primarily through FHIR-based APIs, allowing patient records, appointment data, and clinical documentation to sync between the telemedicine platform and the hospital’s system of record without manual re-entry.
Why interoperability matters clinically, not just technically
A telemedicine visit that never updates the patient’s permanent medical record creates a fragmented care history. HL7 is the older messaging standard still used in many legacy hospital systems. FHIR is the modern, API-based standard most current integrations are built around. SMART on FHIR adds an authorization layer that lets a telemedicine app launch securely from within an EHR’s existing interface rather than as a disconnected tool.
What actually gets synchronized
Integration covers several data flows: patient synchronization, appointment synchronization, clinical documentation written back into the chart, medication updates reflected in both systems, and lab results syncing bidirectionally.
The real integration bottleneck
The technical API work is well documented at this point, since FHIR is a mature standard. The harder part is the certification and approval process each EHR vendor requires before granting production access.
A second common challenge is data mapping. A telemedicine platform’s data model rarely lines up cleanly with the EHR’s internal structure. It requires careful field-by-field reconciliation rather than a simple pass-through connection.
How Can Telemedicine Apps Improve ROI and Patient Outcomes?
Telemedicine apps improve ROI by reducing no-show rates and raising clinician utilization, while improving patient outcomes through better follow-up adherence and faster access to specialists, but these benefits depend on deliberate workflow design, not on the technology alone.
1. Business outcomes
Reducing no-shows is one of the most measurable financial benefits of virtual care. A retrospective study across a large safety-net health system, covering more than 355,000 patients and 2.6 million outpatient encounters, found that telehealth visits were associated with a 29% reduction in the odds of a no-show compared to in-person visits.
That reduction translates directly into better clinician utilization, since scheduled time is used more consistently rather than lost to empty slots.
McKinsey has separately estimated that as much as 30% of Medicare fee-for-service and Medicare Advantage acute-care spending could potentially be delivered at home, which signals the scale of the operational shift health systems are underwriting when they invest in virtual care infrastructure.
2. Clinical outcomes
Telemedicine’s clinical value is strongest in chronic disease management and behavioral health, where continuity of contact matters more than any single encounter.
A systematic review of patient satisfaction across telemedicine studies found that improved clinical outcomes were the benefit most frequently reported, cited in over half of the studies reviewed, alongside measurable gains in patient satisfaction scores. Because follow-up visits carry less friction for patients, adherence to recommended check-ins tends to improve.
One documented example: An academic psychiatry practice tracked no-show rates across roughly 13,000 scheduled visits per period before and during its shift to telehealth, and found the overall clinic no-show rate dropped from 18.1% to 15.3% after the transition.
The same research flagged digital literacy, on both the patient and provider side, as a critical factor in realizing that improvement. It is a reminder that the technology enables the outcome, but proper onboarding is what actually delivers it.
Access to specialists improves most clearly for patients outside major metro areas, where a virtual consultation removes what would otherwise be a multi-hour drive to see a subspecialist.
What Should You Look for in a Telemedicine App Development Company?
Organizations should evaluate a telemedicine app developer on healthcare domain expertise, regulatory understanding, security track record, interoperability experience, and architecture quality.
Each of these criteria maps to a specific risk that generic software vendors often underestimate.
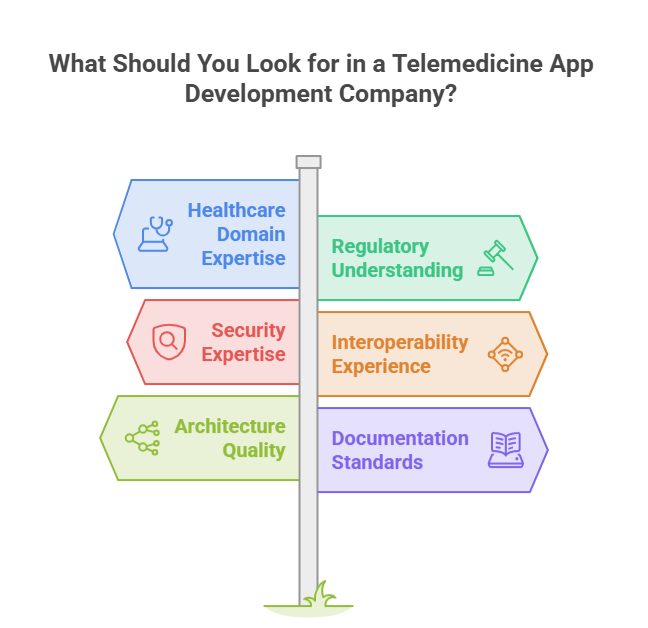
Healthcare Domain Expertise
It matters because clinical workflows carry constraints, like licensure boundaries, documentation requirements, consent rules, that a team without healthcare experience typically discovers only after launch, when they’re expensive to fix.
Regulatory Understanding
It should be demonstrated through specifics: how a partner has previously structured BAAs, handled state-level telehealth licensure differences, or scoped GDPR requirements, rather than a general claim of “HIPAA compliance.”
Security Expertise
It should include a track record of independent penetration testing and risk assessments, since self-assessed security claims carry limited weight on their own.
Interoperability experience
It is specifically, prior FHIR or HL7 integration work with Epic, Cerner, or similar systems, indicates the team understands certification timelines and data-mapping challenges before they become project delays.
Architecture Quality and Scalability Planning
They determine whether the platform can grow without a costly rebuild; a useful question is how the proposed system would handle a tenfold increase in concurrent video sessions.
Documentation Standards and Post-Launch Maintenance
These commitments matter because healthcare software has a longer operational life than most consumer apps, and undocumented systems become expensive to modify years later.
A relevant healthcare portfolio and a transparent development methodology, such as clear sprint cadence, defined compliance checkpoints, offer a realistic picture of how the engagement will actually run.
Why Software Orca Is a Trusted Telemedicine App Development Company
Building a successful telemedicine platform requires far more than secure video calling. It demands expertise in healthcare workflows, interoperability standards, regulatory compliance, and scalable software architecture.
Software Orca combines these capabilities to deliver telemedicine app development solutions that prioritize security, usability, and long-term growth.
From HIPAA-ready architectures and FHIR-based integrations to intuitive patient experiences and provider-focused workflows, the team develops platforms tailored to real healthcare challenges.
Backed by extensive experience in custom software development and mobile app development services in Dallas, Houston, and other global regions, Software Orca helps healthcare organizations build reliable digital health solutions that support better care delivery, operational efficiency, and future scalability.
Wrapping it Up
Telemedicine app development succeeds when architecture, security, and compliance are treated as foundational decisions rather than late-stage additions.
Platforms that hold up combine well-planned system architecture, strong technical safeguards, genuine HIPAA and GDPR compliance, real EHR interoperability through FHIR and HL7, technology choices matched to actual scale and team capability, and design that follows real clinical and patient workflows rather than a generic template.
The technical decisions made early in development determine the platform’s cost, security posture, and clinical usefulness for years afterward, and with reimbursement policy now more stable than it has been in years, the organizations that get the architecture right first will be the ones positioned to scale it.

Frequently Asked Questions
How long does telemedicine app development take?
A basic MVP typically takes 3 to 5 months, a mid-sized platform 5 to 9 months, and an enterprise system with full EHR integration and multi-region compliance 9 to 18 months. Timeline is driven primarily by integration complexity and compliance review, not raw feature count.
Can a Telemedicine App Work Without an EHR Integration?
Yes, a telemedicine app can function without integrating with an EHR system, particularly for startups, independent clinics, or organizations launching a minimum viable product (MVP). Core features such as appointment scheduling, video consultations, secure messaging, and online payments can operate independently. However, as the platform grows, EHR integration becomes increasingly important for synchronizing patient records, prescriptions, lab results, and clinical documentation.
Do Telemedicine Apps Require FDA Approval?
Most telemedicine apps do not require approval from the U.S. Food and Drug Administration (FDA). Applications that facilitate video consultations, appointment booking, messaging, or electronic prescriptions are generally not regulated as medical devices. However, if a telemedicine app includes features that diagnose diseases, recommend treatments, analyze medical images, or perform other clinical decision-making functions, it may qualify as Software as a Medical Device (SaMD) and become subject to FDA oversight.
Can AI Be Integrated into an Existing Telemedicine App?
Yes. Many healthcare organizations introduce AI capabilities after launching their initial platform rather than building them from day one. Common enhancements include AI-powered medical transcription, automated clinical documentation, appointment summaries, symptom assessment, intelligent scheduling, and patient engagement chatbots. AI integration into an existing application typically requires API integrations, secure access to healthcare data, model validation, and ongoing monitoring to ensure accuracy, privacy, and regulatory compliance.
How Do Telemedicine Apps Handle Poor Internet Connections During Video Consultations?
Reliable telemedicine platforms are designed to maintain consultation quality even when network conditions fluctuate. Modern video solutions typically use adaptive bitrate streaming to automatically adjust video quality based on available bandwidth. Additional techniques such as automatic reconnection, TURN/STUN servers for NAT traversal, packet loss recovery, and audio-first fallback help minimize disruptions during consultations.
Can a Telemedicine App Support Multiple Medical Specialties on a Single Platform?
Yes. Modern telemedicine platforms are commonly built to support multiple specialties, including primary care, mental health, dermatology, cardiology, pediatrics, and other clinical services within a single application. This typically requires a flexible architecture that supports specialty-specific consultation workflows, customizable clinical documentation templates, role-based access controls, scheduling rules, and billing configurations.